
CAUGHT IN THE MIDDLE
High-conflict divorce and psychotherapy
Case 4
Let’s look at an example of a therapist who sees a child whose parents are in the process of divorce, and gets involved with the court. Such therapists generally want to be helpful, to their clients, to the courts.Some feel an obligation to advocate for their clients. But this is where, in my experience, therapists most often run into trouble.
A psychologist is referred an adult woman by a child custody evaluator. The evaluator recommended treatment for her with the hope that in six months he can recommend joint custody. In many ways the parents are equal in their parenting capacity and both have been very involved with the child. Parenting time is equal between the parents.
The mother, per the evaluator, suffers from an anxiety disorder, interfering with her ability to separate from her 2- year old child. This led to her making an abuse allegation: when dad was taking the child out of town, she brought the child to the doctor saying that the child had an ear infection and shouldn’t’t fly. The doctor didn’t agree. She then took the child to an urgent care facility trying to get a doctor to write a note saying the child couldn’t fly.
That doctor refused. She then took the child to the first doctor saying that the child had told her that his father had hit him in the stomach. The doctor was a mandatory reporter and contacted CPS. CPS did not substantiate, worked quickly, and did not block the Xmas trip.
During a custody evaluation, mom accused the dad of repeatedly abusing her, including knocking her down when she was pregnant with the child. Medical records and statements from her friends and family indicated that she never accused her husband until the divorce was filed. In the context of what happened around dad’s trip, and in light of dad’s psychological evaluation, this allegation could not be credited.
Testing and clinical observations suggested that mom’s anxiety about separation from her child were behind her allegations. Six-months after referring this mom for treatment, the evaluator meets with mom and then speaks with her therapist.
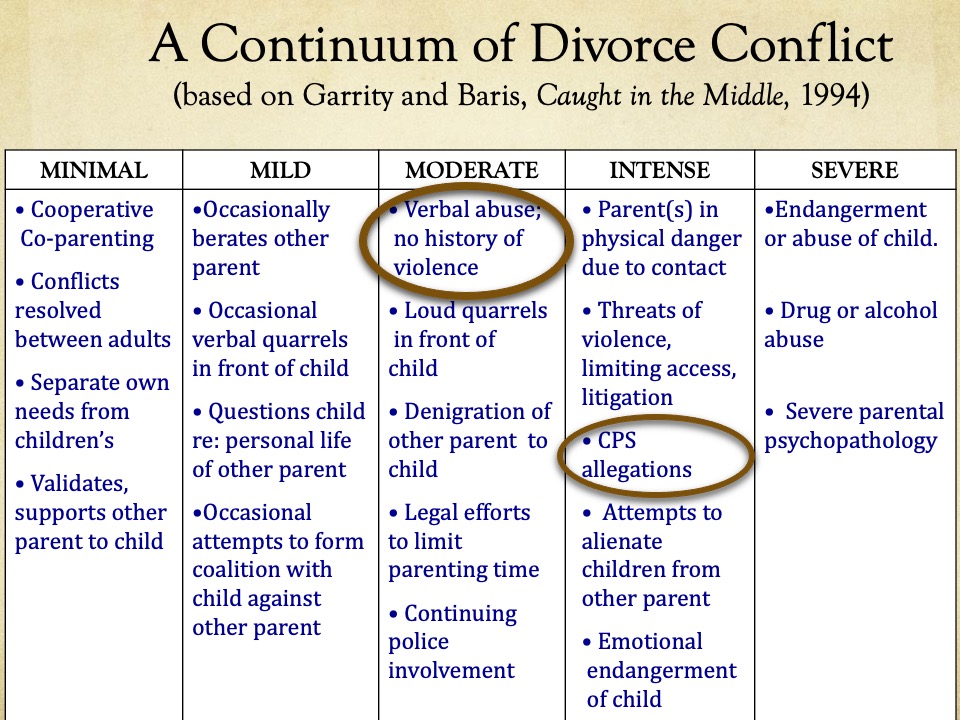
So, for this case, I believe there is a history of verbal abuse, loud quarrels in front of the child and unsubstantiated CPS allegations. There may have been a history of violence, and I had concerns about mom’s capacity for alienating the child from the father. So here we have a case that varies between the moderate and intense levels of conflict.
The therapist says, when the evaluator calls him, that he believes that mother does not suffer from an anxiety disorder. Instead of an anxiety disorder, he felt his patient was “rationally concerned about the child being with an abusive ex-spouse.” His client was legitimately afraid of her husband. “There is no question in my mind there’s been abuse…” Dad had abused the mom financially and physically, he stated.
The therapist expressed a number of very negative attitudes about the ex-husband; whom he described as “critical,” “demeaning,” and “negative.”
This therapist never met the ex-husband/father.
The Therapist “did not believe that anyone could make up” all of the things which his client had said to him about her husband. Mom’s anxiety about separation from her son was due, in the therapist’s opinion, to fear and intimidation in response to the abusive father; it was a rational response. His treatment had focused on helping his patient to stand up to this man whom he believed to be physically and emotionally abusive.
The child, he said, had told his mom that his dad did not let the child talk to her, that his dad plays rough, that his dad didn’t like mom, that his dad thinks that the child is “ugly.” The therapist believes that these reported statements by the child (whom he also has not seen) were prompted by his dad. The Dad (had reportedly) referred to the mom as a ‘crazy…a freak…a bad wife…fat…’ and ‘ugly,’ according to the therapist .
This therapist sees his client as the victim and her ex-husband as the aggressor. He promised to write a letter or testify in court.
The evaluator was “obviously wrong in his assessment of my patient,” he said. He was ready for a battle.
Who is the client?
- Therapist: The mother. He is not objective, has not met or evaluated the father.
2. Custody evaluator: The court, the child(ren)
What ethical principles are involved/appear to being violated?:
9.01 Bases for Assessments : “…psychologists provide opinions on the psychological characteristics of individuals only after they have conducted an examination of the individuals adequate to support their statements or conclusions…(b) … psychologists provide opinions of the psychological characteristics of individuals only after they have conducted an examination of the individuals adequate to support their statements or conclusions. …
3.05 Multiple Relationships::… A multiple relationship occurs when a psychologist is in a professional relationship with a person and at the same time is in another relationship with the same person…
A psychologist refrains from entering into a multiple relationship if the multiple relationship could reasonably be expected to impair the psychologist’s objectivity, competence or effectiveness
Which statements by the therapist are ethically legitimate?
Who could be harmed?
- The child
2. The father
Ask yourself:
What should a therapist do in this situation?
What pitfalls does he need to avoid?
Special considerations for court-involved roles with children:
(a) When children are to be involved in treatment, the CIT has an enhanced obligation to avoid biasing conditions in their work such as involvement with only one parent, and must be alert to biasing conditions that may be outside of the CIT’s control.
Examples include missing information, external influences on a child, or other exposure to the parental conflict.
(b) Children’s behavior and statements may vary markedly based on the circumstances of treatment.
(c) The CIT has an enhanced obligation to consider multiple treatment hypotheses and be knowledgeable about children’s developmental tasks and needs.
(d) The CIT should use particular caution to ensure that he/she has adequate data on which to base any opinions or assessments, and to form and express such opinions only within confines of the therapeutic role and available information
What statements, actions would remain within the therapeutic role?
(e) The therapist must use particular caution in considering statements by children that express positions on adult issues, to avoid inaccurate or incomplete assessment of a child’s needs and feelings; for example, when children say what custody arrangement they want.